The quick version
- A recent report from the Rochester Beacon looks at how AI is being used in radiology departments, mostly behind the scenes to draft report summaries and pull up old imaging history.
- The radiologists interviewed are clear that the software does not diagnose on its own. A human still reads the images, edits the report and signs off.
- One of the biggest reasons hospitals are interested is a real shortage of radiologists, paired with more people needing scans than ever.
- Researchers are honest about the risks: AI can fail in odd ways, and people can lean on it too heavily without realising.
- For patients, the part that hurts most is rarely the technology. It is the wait, and that is the problem mobile imaging was built to chip away at.
You have probably done it. A strange pain shows up, you reach for your phone, and you type your symptoms into a search bar or a chatbot before you even think about ringing your GP. Most of us want answers fast, especially when something feels wrong. So it is worth asking what happens once the question moves past your phone and into a real radiology department, where AI tools are now quietly part of the picture.
A thoughtful piece by Rob Bell for the Rochester Beacon, titled Radiology in the age of AI, walks through exactly that question. It follows a patient stuck in a painful waiting game and talks to the radiologists and researchers working out where these tools belong. We read it from the perspective of a mobile imaging provider here in Brisbane, and a lot of it rang true. Here is what stood out.
The waiting is the hard part
The story opens with Meghann Maiellano, a 41-year-old inpatient psychiatric nurse who developed intense, knife-like pain in her abdomen along with bad cramping. Her first thought was the obvious one many of us would land on: "I thought it was my appendix."
Her doctor referred her to a specialist, who sent her for an urgent CT. It still did not pinpoint what was wrong, and she then faced a wait of several weeks before she could get any further scans. A trip to the emergency department led to more of the same: more waiting, no relief from the pain, and mounting frustration. Months later she had a colonoscopy, then weeks after that an ultrasound. Doctors suspect the trouble may stem from her gallbladder, or possibly an inability to process fructose, but more tests are still needed to be sure. The pain has not fully gone.
What she points to is not a diagnosis gone wrong. It is the gap between scans. "It was the time it took to get these tests," she says. "Not knowing what's wrong, the pain." That is the bit worth holding onto as the article gets into the technology. The frustration that wears people down is usually about access and timing, not whether a clever piece of software helped write the report. Maiellano said she would support AI if it helps patients like her get answers sooner, though as a general idea she still finds it, in her word, "terrifying". Both things can be true at once.
What AI is really doing in radiology
Here is the part that surprised us a little, in a reassuring way. At the University of Rochester Medical Center, which the article says serves around a million patients a year, the AI in radiology is far more modest than the headlines might suggest. It mostly helps with paperwork.
Sean Cleary, a cardiothoracic radiologist and vice chair of informatics at the medical centre, explained that the department has long used a dictation platform where the radiologist views the scan on one monitor while speaking the report into a program running on a second. The AI layer is recent. "PowerScribe is basically just the dictation platform," he says. "The AI part of it only started within the last two years."
One feature drafts the short summary that sits at the end of a report, the part that pulls together the key conclusions. It does not look at the scan itself or form its own opinion; after the radiologist describes what they see, the software tidies that into a summary. As Cleary puts it, "the impression section, for lack of a better expression, is like a TLDR of the report. What they're really good at is summarizing information. They're not doing independent thought."
Another tool being piloted condenses a patient's older radiology reports so the radiologist can catch up quickly, and it shows where each point came from. "It gives you a clickable link to each sentence that it's getting the summary from," Cleary says, "so I know what the provenance of that information is." So for now, as he put it, "for the average patient right now, a lot of it's behind the scenes". The gains are incremental, roughly five percent, but they add up across a long day of reading scans.
One worth watching: The article also describes software that can spot signs of a stroke and push that study toward the front of the line, so a radiologist reads it sooner. Gregg Nicandri, the medical centre's chief medical information officer, framed it as spotting "opportunity for early intervention where it changes the outcome for the patient". In mammography, AI may help flag the need for extra views while the patient is still on site, which, as he said, could "save them the extra visits, save them the anxiety".
The radiologist stays in the loop
If there is one line from the piece worth remembering, it is Cleary's description of who is actually responsible for the result: "the ultimate guardrail is the radiologist." Radiologists still interpret the images, review anything the software produces, edit the report and give final approval.
Nicandri described a careful process before any tool gets switched on. "We kind of take an evidence-based approach to anything we deploy," he says. "We want to make sure that it works and it's safe before we just turn it on." He also described an internal policy that keeps patient information out of public AI tools, with secure internal versions instead, where "any information that gets put in there, we control and protect. It's not used to train the larger model." That matters, because privacy worries are one of the most common questions patients raise when AI and health records come up in the same sentence.
It is a point worth sitting with for a moment. A signature on a radiology report is not just a formality. It is a person taking legal and professional responsibility for the reading. Software can draft, summarise and flag, but it cannot stand behind a diagnosis the way a clinician does. The human in the chair still owns the result, and that ownership is what keeps the whole system accountable.
What the experts are worried about
The article does not pretend the technology is risk-free, and neither will we. Ashique Khudabukhsh, an AI researcher at the Rochester Institute of Technology, raised the kind of failure that is hard to predict. "The biggest risk that I see is that when you have systems that are very complex and not easy to understand, they can fail in very unexpected ways," he says. "We understand human failures much, much better because we have been doing this for ages."
He put it more plainly too: "You can have LLMs that can write a fancy poem, and then cannot count." His team ran a study using a framework they call HAUNT. They had five chatbots write both accurate and inaccurate claims about famous films and books, then gently steered them toward the wrong answers. Not one of the models held its ground reliably, and a couple of them, Gemini and DeepSeek in particular, went along with and echoed the false claims in roughly half of cases once the prompting got subtle. The worry in a clinical setting writes itself: "What if it just inserts one sentence which maybe the doctor did not intend to say?"
Then there is the human side of overreliance. Khudabukhsh described what happens when trust in a tool deepens because it usually performs well: "At some point, there is kind of a cognitive unloading. I am transferring the thinking load on the machine." Nicandri raised the same theme from the training angle, asking how you teach the next generation of radiologists to use these tools without becoming dependent on them. His answer was that you keep "the expert human in the loop". A 2024 study from Harvard Medical School, MIT and Stanford, cited in the article, reviewed how 140 radiologists handled 15 different chest X-ray reading tasks. The result was mixed: AI lifted some readers' performance and dragged others' down. The interaction between a person and the machine is not one-size-fits-all, and the researchers admitted it is not yet fully understood.
Speed, safety and the shortage problem
So why push ahead at all? Cleary gives the honest reason, and it is the one that maps most directly onto our own world: "the lack of radiologists is a major driver." Imaging has become more central to medicine. Cancer care now leans heavily on scans, organised screening such as lung cancer checks has expanded, and the machines themselves have improved. All good news for patients, and all of it adds load onto a workforce that is already stretched. That pressure is exactly what Meghann Maiellano felt as weeks-long gaps between her scans.
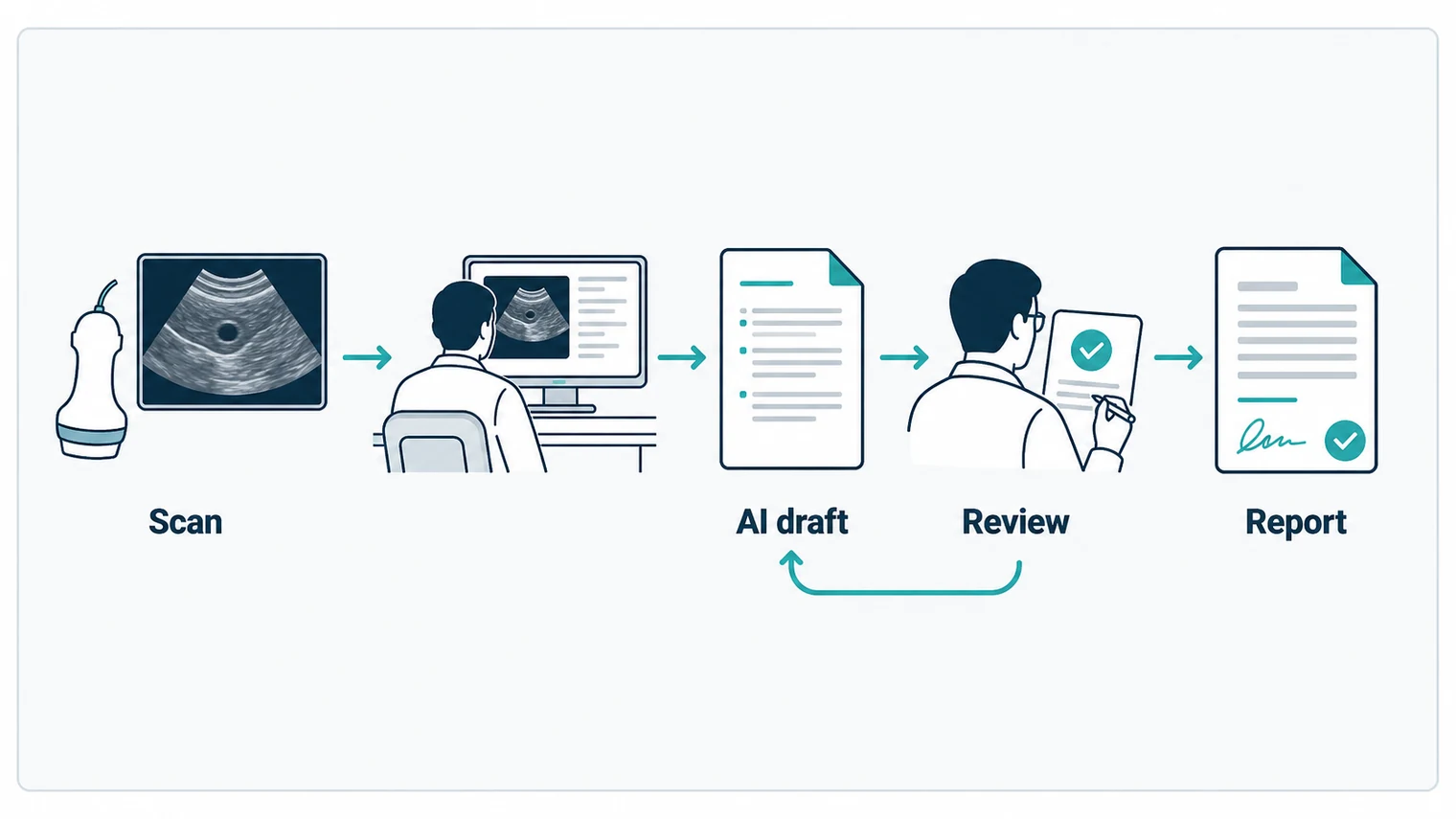
Cleary reframes the usual fear in a way that stuck with us, pointing out that the risks run in both directions. "Everyone always thinks about the risks of using it," he says, "but you also have to think about the risks of not using it, because things are gonna get missed as well." Used narrowly, to summarise accurately, pull up history quickly and avoid omissions, he sees it as both an efficiency tool and "ironically, it's also kind of a patient safety tool". The table below sums up the rough split the article describes between what these tools are doing today and what they are not.
| What the AI does today | What it does not do |
|---|---|
| Drafts the short summary from what the radiologist already dictated | Read the scan and form its own diagnosis |
| Condenses old reports and links back to the source | Replace the radiologist's review or signature |
| Flags urgent cases to be read sooner | Make the final clinical decision |
| Helps catch the need for extra views on site | Get used with patient data on public tools |
What we make of it at Modia
We are a mobile imaging team. We bring X-ray and ultrasound to people's homes and into aged care, so we will be upfront: we do not use the specific tools named in this article, and the report describes a large American academic hospital, not the Australian system. What drew us to it is the underlying problem, because it is the same one we work on every day. People in pain wait too long for scans, and the workforce that reads those scans is under strain.
That shortage is not just an overseas story. When a resident in aged care or someone with limited mobility needs imaging, the trip to a hospital department can mean ambulance transfers, long waits and real distress, sometimes for a scan that takes minutes once it starts. Reducing that friction is the whole point of mobile imaging. AI in the reporting room and mobile imaging at the bedside are aiming at the same goal from different ends: getting a clear answer to the right clinician faster, without cutting the human expert out of the decision.
Cleary made one more point we agree with. People are already asking chatbots about their symptoms, and the replies can be clearer than a basic web search, but "you still need to talk to your doctor". A summary, whether it comes from a chatbot or a clever piece of reporting software, is a starting point. The diagnosis still belongs to a qualified human who takes responsibility for it. As Maiellano said, she would like to keep her faith in the health system. The way to earn that, on both sides of the world, is to use new tools where they genuinely help and to be honest about where they do not.
Need imaging without the long wait?
For Home Visits:
Book Home Ultrasound – imaging in your own space
For Aged Care Facilities:
Book Facility Visit – bedside imaging without a hospital transfer
This article is general information, not medical advice. If you have symptoms that worry you, or you are waiting on imaging and your pain is getting worse, please speak with your GP or treating doctor. They can advise what testing you need and how urgently.
Source: this post discusses and responds to Radiology in the age of AI by Rob Bell, published by the Rochester Beacon on 28 May 2026. All quotations belong to the people named in that article. Modia Health has no affiliation with the Rochester Beacon, the University of Rochester Medical Center or the products mentioned.