Dealing with uncomfortable bowel symptoms and wondering if ultrasound will give you the answers you need? Here's what nearly 8 years of sonography practice has shown our team about what ultrasound can, and can't, detect.
The Real Talk
Yes, abdominal ultrasound can detect many bowel problems, though it has real limits. Think of it as a strong first step in your diagnostic journey, not necessarily the final word.
The Clinical Advantage of Bedside Assessment
Across years of mobile practice in Brisbane, our team has noticed that bowel assessments often work better when patients are scanned in their familiar environment. The reason is physiological. When a patient is relaxed, with no ambulance transfer or hospital waiting room hanging over them, their abdominal muscles are less guarded, and that gives sonographers clearer diagnostic windows.
Unlike CT or MRI scans, which capture static snapshots, ultrasound lets us visualise peristalsis in real time. You don't just see the anatomy. You see the function. We can watch exactly how the bowel is moving (or struggling to move), which matters for telling mechanical obstructions apart from functional issues like ileus.
The Fasting Question Everyone Asks
Here's where it gets a bit, well, complicated. And honestly, this part confuses most patients (and quite a few new sonographers) at first.
For most abdominal ultrasounds, you'll be asked to fast for 4-6 hours beforehand (4 for diabetics). The reason? Gas in your bowels can block the view. Sound waves don't travel well through gas, so a gas-filled bowel can make an examination non-diagnostic.
Fasting Guidelines
- General abdominal scan: Fast 4-6 hours
- IBD monitoring: No fasting required, eat and drink normally
- Emergency scans: Performed regardless of fasting status
But (and here's the interesting part) when sonographers are specifically monitoring inflammatory bowel disease, we actually encourage you to eat and drink beforehand. Why? Because the focus is on specific findings like bowel wall thickness and inflammation patterns, not trying to see everything sitting behind your bowels.
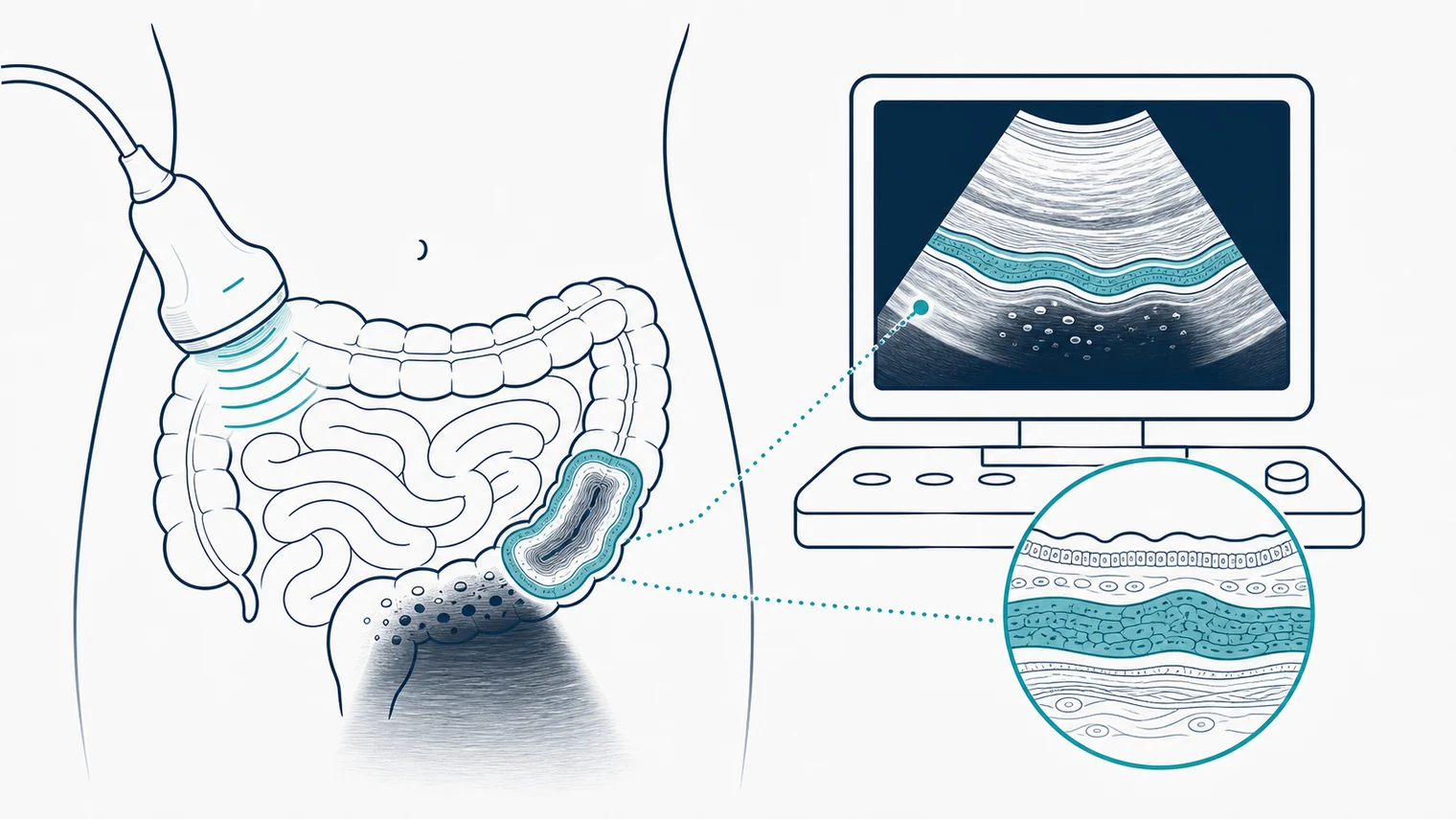
What We Actually See When We Scan Your Bowels
- Bowel wall thickening (>4mm concerning)
- Increased blood flow on Doppler
- Loss of normal bowel wall layers
- Mesenteric fat inflammation
- Dilated bowel loops (2.5cm)
- Abnormal "back-and-forth" peristalsis
- Fluid between bowel loops
- Collapsed distal bowel
- Appendix wider than 6mm
- Non-compressible appendix
- Target sign in cross-section
- Periappendiceal fluid
- Bowel wall thickening (4mm)
- Inflamed pericolic fat
- Visible diverticula
- Abscess detection
Inflammatory Bowel Disease (IBD), Crohn's and Ulcerative Colitis
This is where ultrasound really shines. It's become a go-to tool for monitoring disease activity in patients with Crohn's and ulcerative colitis, particularly useful because it can be repeated as often as needed.
Most studies (75%) consider bowel wall thickness >3mm as abnormal. Normal bowel walls are typically less than 2mm.
That makes ultrasound a strong fit for tracking treatment response over time, since you can have multiple scans to check whether your therapy is working.
Bowel Obstructions, When Things Get Blocked
Our sonographers see this condition often, especially in aged care. Research shows ultrasound performs comparably to CT imaging for detecting small bowel obstructions, making it a strong choice when you want to avoid the emergency department.
A key advantage here is that patients can be monitored conservatively, with treatment progress tracked over multiple scans and no radiation concerns to worry about.
Appendicitis, The Classic Emergency
Appendicitis is where the safety advantages of ultrasound become most clinically relevant. CT scans are technically more accurate (94% vs 75-90%), but the trade-off matters.
The Clinical Trade-off
For most adults, a negative ultrasound followed by clinical monitoring is often enough. If uncertainty remains, CT can be ordered, but ultrasound often provides the answer without needing to escalate.
Diverticulitis, When Those Little Pouches Act Up
In Europe and Asia, ultrasound is routinely the first choice for diverticulitis, and that practice is gaining traction in Australia too. It's particularly useful for telling uncomplicated cases (that can be managed at home) apart from those needing hospital admission.
The Honest Truth About Limitations
Time to be completely upfront with you. Ultrasound isn't perfect. As a team that does this every day, we want you to understand exactly what sonographers are up against.
Challenges
- Bowel gas can block the view
- Higher BMI may reduce image quality
- Operator skill heavily affects results
- Can't see microscopic inflammation
- Cannot replace endoscopy for biopsy
Advantages
- See peristalsis in real time (unique to ultrasound)
- Portable, scans happen where you are
- Same-day or next-day availability
- Results discussed immediately
- Cost-effective triage tool
Our Equipment: Our ultrasound machine is about the size of a chunky laptop, and our team literally carries it in with a backpack. We use GE Healthcare ultrasound units, the same technology our clinical lead has trained sonographers on across Queensland while working as an application specialist.
Body habitus matters. Mobile machines are smaller than hospital units. For most patients, there's no image quality difference at all. For high BMI patients, our team might see about a 10% reduction in image quality, still diagnostic in most cases, though occasionally we'll recommend a hospital-based scan for definitive answers.
Operator skill carries real weight. Unlike automated blood tests, ultrasound interpretation depends heavily on who's performing the scan. Our accuracy stays high because we use very experienced technicians who've worked in hospital settings, so they're used to similar patient types, pathologies, and limitations. When there are limitations on the imaging, our radiologists clearly outline that in the report.
When Ultrasound Isn't Enough
Sometimes the honest answer is, "We need more information." Ultrasound can't replace endoscopy for initial IBD diagnosis. You need a tissue biopsy for that definitive answer. And for some conditions, CT or MRI may provide extra information that ultrasound simply cannot give.
Contrast-enhanced ultrasound uses tiny gas bubbles in your bloodstream to highlight blood flow patterns. Artificial intelligence is being developed to help standardize what we see and reduce operator dependence.
What This Means for You
If you're dealing with ongoing bowel issues, ultrasound is often your safest first step, a way to get answers without the stress and wait times of hospital emergency departments.
Initial screening to determine if hospital attendance is actually necessary
Ongoing monitoring for chronic conditions without repeated hospital visits
Real-time assessment for when dynamic bowel function matters
What Hospital Transfer Actually Looks Like
Our sonographers see this play out often when elderly patients get transferred. Instead of staying in their bed or sitting in their chair, they may need a hoist to get onto a stretcher. Then from stretcher onto an ambulance. Then from ambulance to a hospital bed. Then from hospital bed to an ultrasound room bed.
What if they're already in pain from a suspected fracture or abdominal issue? They're getting shuffled around, and going to hospital doesn't mean you get your scan straight away. Sometimes you wait several hours. Sometimes all day for an ultrasound.
And after all that? They might just come back to the aged care home in the same pain, with the same questions, because the scan didn't find anything that changes immediate management.
Our team often scans patients in aged care who are so relieved they didn't have to go to hospital. Their families are grateful too. We've saved them from taking half a day off work, fighting traffic, and sitting in waiting rooms. Instead, they can spend that time with their loved one doing something nice.
The Real-World Experience
Here's what our mobile practice commonly sees. The most frequent abdominal requests are query gallstones for abdominal pain, bowel obstruction (especially when there's suspected faecal loading), and excluding cholecystitis. The team also handles urinary obstruction, calculi, and unexplained weight changes.
One advantage we have: we adapt to where the patient is. If they can't sit up, sonographers can scan them lying in bed and just raise the head of the bed for better positioning. Our techs are used to these challenges from years of hospital work.
The most frequent overall requests are:
Many patients our sonographers scan are confused, wary of anyone they don't know, and distrustful. Going into a clinic and waiting in a dark room with strangers, meeting new people along the way as shifts change, all of that is genuinely daunting.
Here's what research shows: Delirium can kick in within just 3 hours of being in an unfamiliar hospital environment. When that happens, the hospital has to assign a dedicated staff member, which stretches already tight resources even further.
Compare that to mobile imaging. The patient stays in the room they always live in. Same staff they know. One new person who's in and out within 30 minutes. Their favourite nurse can hold their hand through the procedure.
For elderly patients especially, avoiding hospital transfers can be life-changing. Instead of spending 10 hours in a busy emergency department, they get answers in their familiar environment, often within 24 hours of referral.
When to Seek Immediate Help
Don't Wait for an Ultrasound If You Have:
- Severe, sudden abdominal pain
- Persistent vomiting with inability to keep fluids down
- Blood in your stool
- High fever with abdominal symptoms
- Signs of dehydration or shock
These could indicate emergency situations that need immediate hospital attention.
For urgent situations: Contact your GP immediately or call 000 for emergency services.
Mobile Ultrasound: Healthcare That Comes to You
At Modia Health, our mission is to bring diagnostic technology directly to where you need it most.
Additional Resources
Learn More About Our Services:
- Complete Ultrasound Guide, everything you need to know about preparing for your scan
- Mobile X-Ray Services, for when ultrasound isn't enough
- IV Therapy at Home, mobile healthcare solutions across Brisbane
References & Sources
This article is based on peer-reviewed medical research and clinical guidelines. Hover over statistics in this article to see their sources.
Small Bowel Obstruction
- Frasure SE, et al. World J Emerg Med. 2018;9(4):267–271
- European Journal of Radiology. 2021, Meta-analysis
- American Family Physician. 2021;104(2):135-140
Inflammatory Bowel Disease
- Malik S, et al. Ann Gastroenterol. 2024;37(1):54–63
- AGA Clinical Practice Update. Clin Gastroenterol Hepatol. 2024
- Wiley Online Library – J Clin Ultrasound. 2025
Appendicitis & Diverticulitis
- Medicine (Baltimore). 2023;102(13):e33413
- Scientific Reports. 2024, Ultrasound vs CT comparison
- J Sci Med Central Gastroenterol. 2024
This information is for educational purposes only and should not replace professional medical advice. Always consult with qualified healthcare providers for proper diagnosis and treatment recommendations.