
Margaret needed a chest X-ray. By the time she returned from hospital, she had a skin tear on her arm, was deeply confused, and refused to eat for three days. The X-ray was clear. Nothing was wrong with her lungs. But the five manual transfers it took to get that answer had done real damage.
If you work in aged care, you've seen this story play out dozens of times. A resident needs imaging. What should take minutes becomes an all-day ordeal of ambulance waits, unfamiliar hands, and anxious hours wondering what's happening to your resident in an overcrowded ED.
But here's what the research tells us: the risks are far greater than most of us realise.
The Hidden Cost of Every Transfer
Every time you transfer a resident - bed to wheelchair, wheelchair to ambulance, ambulance to ED bed, ED bed to imaging table, and back again - you're rolling the dice. Sometimes nothing goes wrong. But the statistics paint a stark picture:
These numbers represent real people - staff members whose backs give out at 45, residents who never walk again after a transfer-related fall, families who watch their loved ones decline after what was supposed to be a routine trip to hospital.
"I am a 130 kg big man and I am not lifting anyone even if I can. I need to be able to work for at least 20 more years. I can't do that with a broken back."
– Experienced Aged Care Worker
The industry consensus is clear: stop lifting people. Yet every hospital transfer forces exactly that - multiple lifts, multiple risks, multiple chances for something to go wrong.
What Goes Wrong
The injuries happen on both sides of the equation:
- Staff Injuries – Back strains, shoulder injuries, chronic pain that ends careers early. Once injured, many healthcare workers never fully recover.
- Resident Injuries – Skin tears from friction, fractures from falls, joint dislocations from improper technique. Some residents never recover their mobility.
"Resident became bedbound for the rest of her life after a fall during an unsafe manual transfer by agency staff who relied on outdated care plans."
– Aged care worker incident report
Why Hospital Transfers Multiply the Risk

A hospital transfer isn't just one manual handling event - it's a cascade of them. And each transfer happens under conditions that make injuries more likely:
The Transfer Cascade
For a single hospital X-ray, your resident faces:
- Transfer 1: Bed to wheelchair (facility staff)
- Transfer 2: Wheelchair to ambulance stretcher (paramedics)
- Transfer 3: Stretcher to ED bed (ED staff)
- Transfer 4: ED bed to imaging table (radiology staff)
- Transfer 5: Imaging table back to ED bed
- Transfers 6-8: The whole process in reverse
That's 5-8 manual handling events minimum - each one performed by different people who don't know your resident.
The Information Gap
Perhaps the most dangerous aspect of hospital transfers is what hospital staff don't know about your residents.
"For elderly ED patients with pending ultrasounds we would have to scope the chart to see whether they were a fall risk because our triage nurses would lie about them being able to stand up and change out of their pants."
– Hospital Radiographer
Hospital staff don't have access to your mobility assessments. They don't know which positions cause pain. They don't recognise the non-verbal cues that tell you a resident is becoming agitated. They're working under time pressure, with unfamiliar patients, often without adequate equipment.
The result? Transfers that would never happen at your facility - where staff know to use the hoist, know to approach from the right side, know that this particular resident needs extra time and reassurance.
What the Research Shows
A major Australian study of 116,192 aged care residents found that the top reasons for hospitalisation directly relate to manual handling:
22.1% of hospitalisations were for injuries, with hip fractures being the most common diagnosis.
And once residents are hospitalised, the complications multiply:
Hospital-Acquired Complications for Aged Care Residents
Percentage of patients affected:
| Complication | Rate |
|---|---|
| Delirium (confusion) | 38% |
| In-hospital mortality | Up to 34% |
| Pressure ulcers | 19% |
Source: Dwyer et al., Age Ageing 2014, Systematic Review
The Irreversible Decline
When transfers lead to hospitalisation, the damage extends far beyond the initial injury:
- Functional decline becomes apparent within 2 days of bed rest
- For hip fractures, only one-third recover their pre-hospitalisation function
- 50-60% cannot walk alone after hip fracture hospitalisation
A Better Approach: Eliminate the Transfer
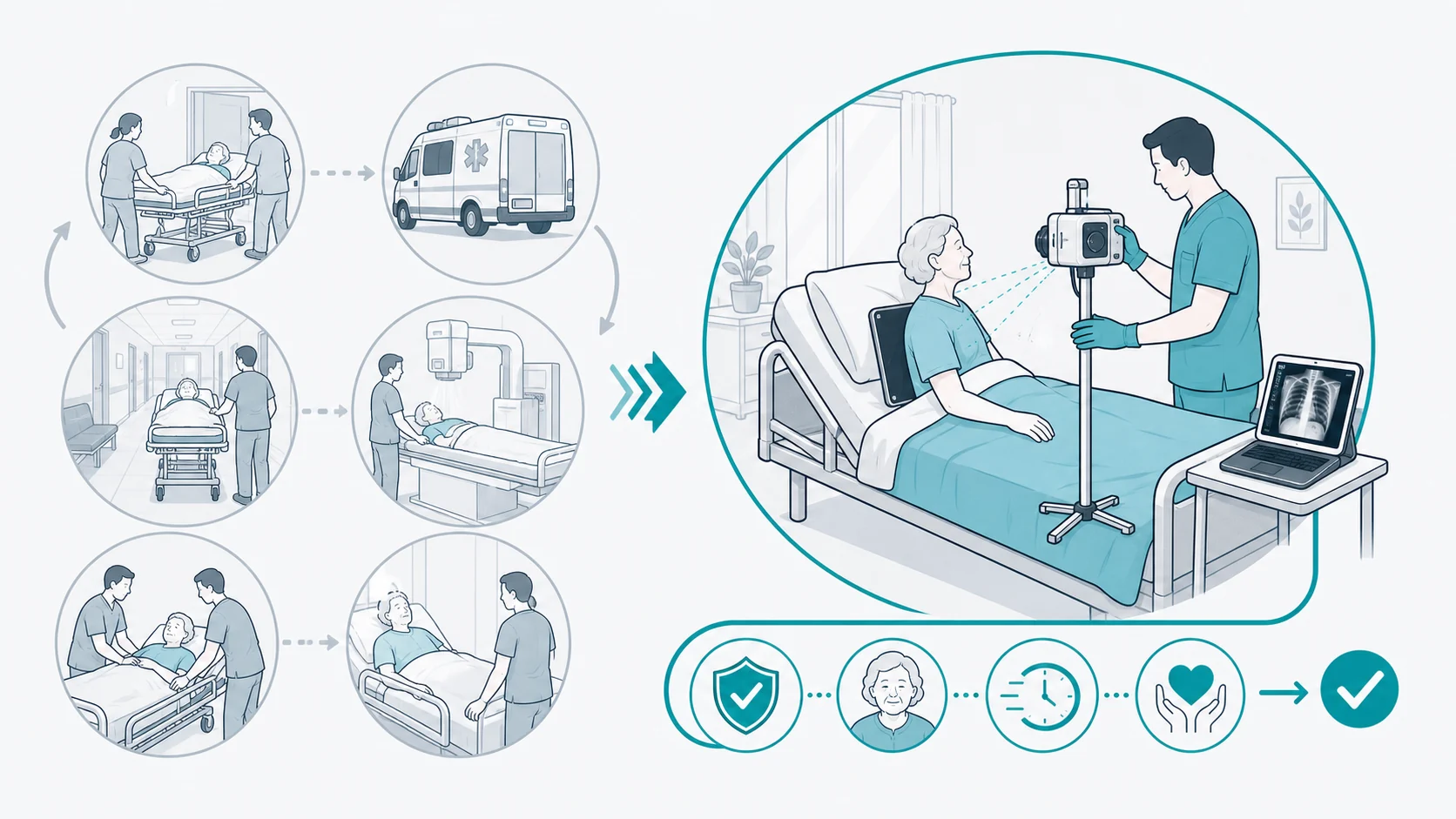
What if, instead of moving the resident to the imaging equipment, we moved the equipment to the resident?
That's the premise of mobile radiology - and it fundamentally changes the risk equation.
Manual Handling Risk Comparison
| Factor | Hospital Transfer | Mobile Imaging |
|---|---|---|
| Number of transfers | 5-8 transfers minimum | Zero transfers |
| Staff performing handling | Multiple unfamiliar teams | Your staff who know the resident |
| Access to care plans | Limited or none | Full access |
| Environment | Unfamiliar, disorienting | Resident's own room |
| Time away from facility | 4-24+ hours | 15-30 minutes |
The resident stays in their bed. Your staff - who know exactly how to position them safely - assist with minor adjustments. The imaging happens in familiar surroundings, with familiar faces, and it's done in minutes rather than hours.
The Evidence for Mobile Imaging
This isn't just theory. The research shows mobile imaging delivers real results:
| Measure | Result |
|---|---|
| Patients who avoided hospital transfer entirely | 25.2% |
| Cost reduction compared to hospital imaging | 85% |
| Manual handling transfers required | Zero |
Clinical Evidence
- Comparable image quality to hospital X-ray - no diagnostic compromise
- Increased diagnostic certainty allowing treatment decisions without transfer
- Faster turnaround - results in hours, not days
Source: Toppenberg et al., 2020 - Mobile X-ray Scoping Review
"It's easier on the patient and no waiting on transport!"
– Radiographer working in mobile services
Making the Change
The path forward is clear: eliminate unnecessary transfers by bringing imaging to the resident.
- Partner with mobile imaging providers. Establish relationships for non-emergency imaging needs before you need them urgently.
- Update your protocols. Make mobile imaging the default for suspected fractures and routine diagnostic needs.
- Educate families. Help families understand that avoiding hospital transfers protects their loved ones.
- Track outcomes. Document transfer-related incidents to build the case for change.
Protect Your Staff and Residents
Modia Health brings X-ray and ultrasound directly to your facility, so there are no transfers, no waiting, and no added risk for your residents.
- Zero manual handling transfers
- Same-day urgent service
- Imaging in their own room
Related Reading
Sources
This article draws on peer-reviewed research and industry data:
Key Research
- Inacio MC, et al. Predictors of hospitalisations and ED presentations shortly after entering RACF. BMJ Open (2021)
- Dwyer R, et al. Systematic review of outcomes following emergency transfer. Age Ageing (2014)
- Toppenberg MD, et al. Mobile X-ray outside the hospital: a scoping review (2020)
Industry Sources
- Safe Work Australia, Manual handling statistics
- Healthcare Australia, Manual Handling Tutorial
- Australian Commission on Safety and Quality in Health Care
This article is for informational purposes for aged care professionals. Clinical decisions should be made in consultation with qualified medical professionals.