You had a fall, or a hard knock, and it still hurts days later. You went for an X-ray and the report came back clear. So why does pressing on that one spot make you wince every time?
Sometimes the answer is a fracture the X-ray could not show. At the Australasian Sonographers Association (ASA) 2026 conference on the Gold Coast, Tabitha Gosden, a general sonographer with more than 13 years of experience and a co-owner of Ultrasound Insight, gave a talk titled "Breaking the norm: Ultrasound's untapped potential for fractures." Her case was that ultrasound can pick up breaks that slip past a normal X-ray, especially in ribs and in children. Here is how, in her words and ours.
The quick version
- Non-displaced fractures, where the bone cracks but does not shift, can be invisible on X-ray.
- Ultrasound reads the surrounding clues: a lifted lining over the bone, a small blood collection, swelling and increased blood flow.
- It detects nearly all rib fractures, compared with less than half on a standard X-ray.
- It uses no radiation and shows the soft tissue at the same time, which makes it useful in children.
When the X-Ray Says Nothing
Ask a room full of sonographers whether you can see a fracture on ultrasound and you will get mixed answers. It depends on training, on the kinds of scans someone does, and even on whether the radiologist they work with believes it can be done. As Tabitha put it, you do not know what you do not know, and there is always more to learn.
Most of us would spot a big, obviously displaced fracture. The skill she was making the case for is catching the subtle, non-displaced ones, where the bone has cracked but stayed in line. Those are the breaks that look normal on an X-ray and keep hurting anyway.
What a Fracture Looks Like on Ultrasound
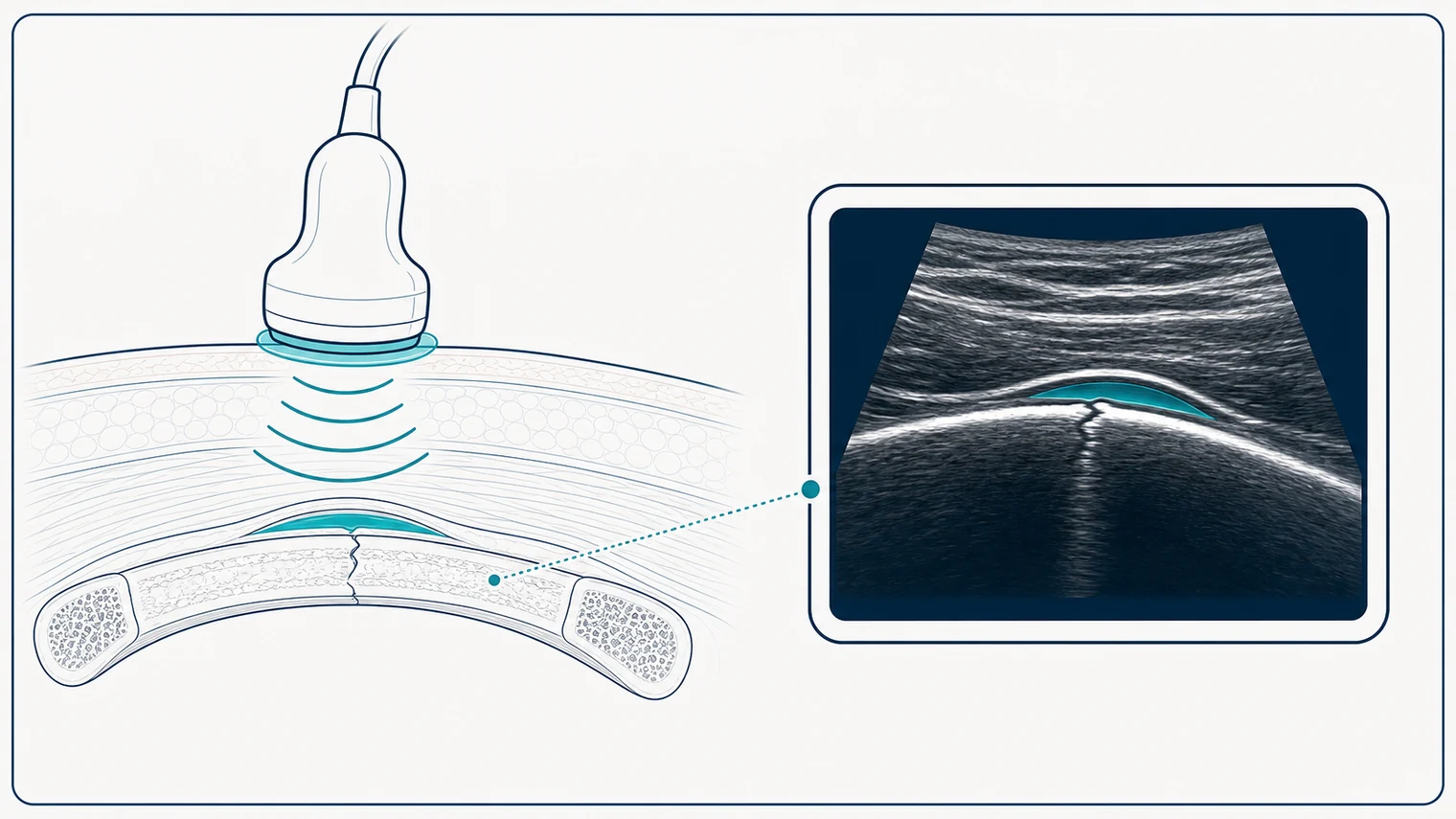
The trick is that ultrasound does not only look for the crack itself. It reads what is happening around it. When a bone breaks, it bleeds. That blood gets trapped under the periosteum, the thin tough layer wrapping the bone, which usually stays intact in a non-displaced fracture.
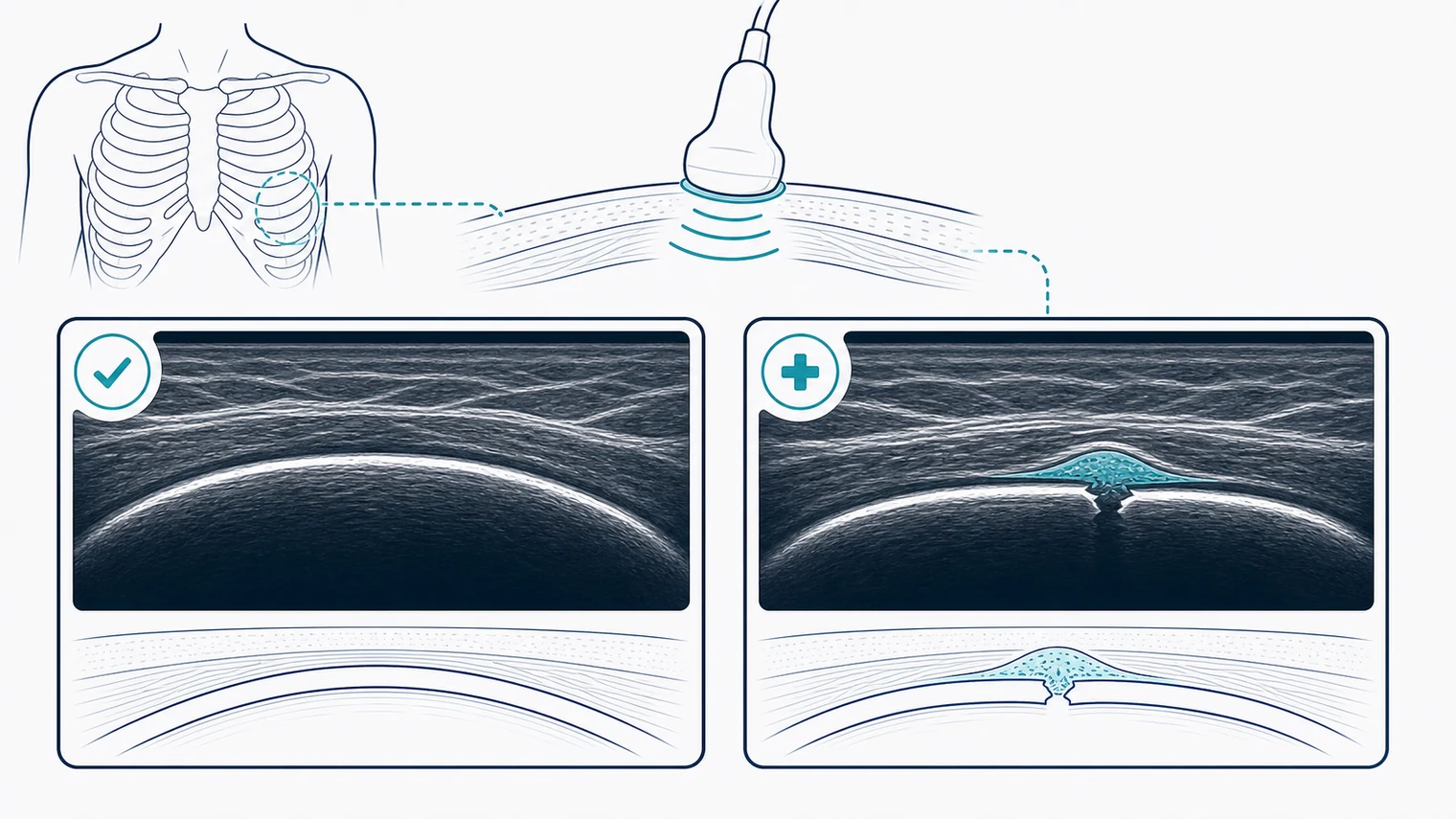
On the screen, that shows up as a dark collection of blood lifting the lining away from the bone. Sonographers call it a periosteal lift, and it is one of the key early clues, sometimes there before you can see any break at all. Alongside it, the scan looks for:
- A step or break in the bone surface – a small interruption in the otherwise smooth bright cortical line.
- Swelling and increased blood flow – the soft tissue around the injury looks puffy and lights up on Doppler.
- Site-specific tenderness – the patient can usually point straight to it, which tells you where to scan.
- Haemarthrosis – blood inside a nearby joint, which matters when the injury is close to one.
Over the following weeks, that early blood collection organises and the body lays down a soft callus that gradually hardens into new bone. So the same spot looks different depending on whether the injury is fresh or healing, which is why knowing the history matters.
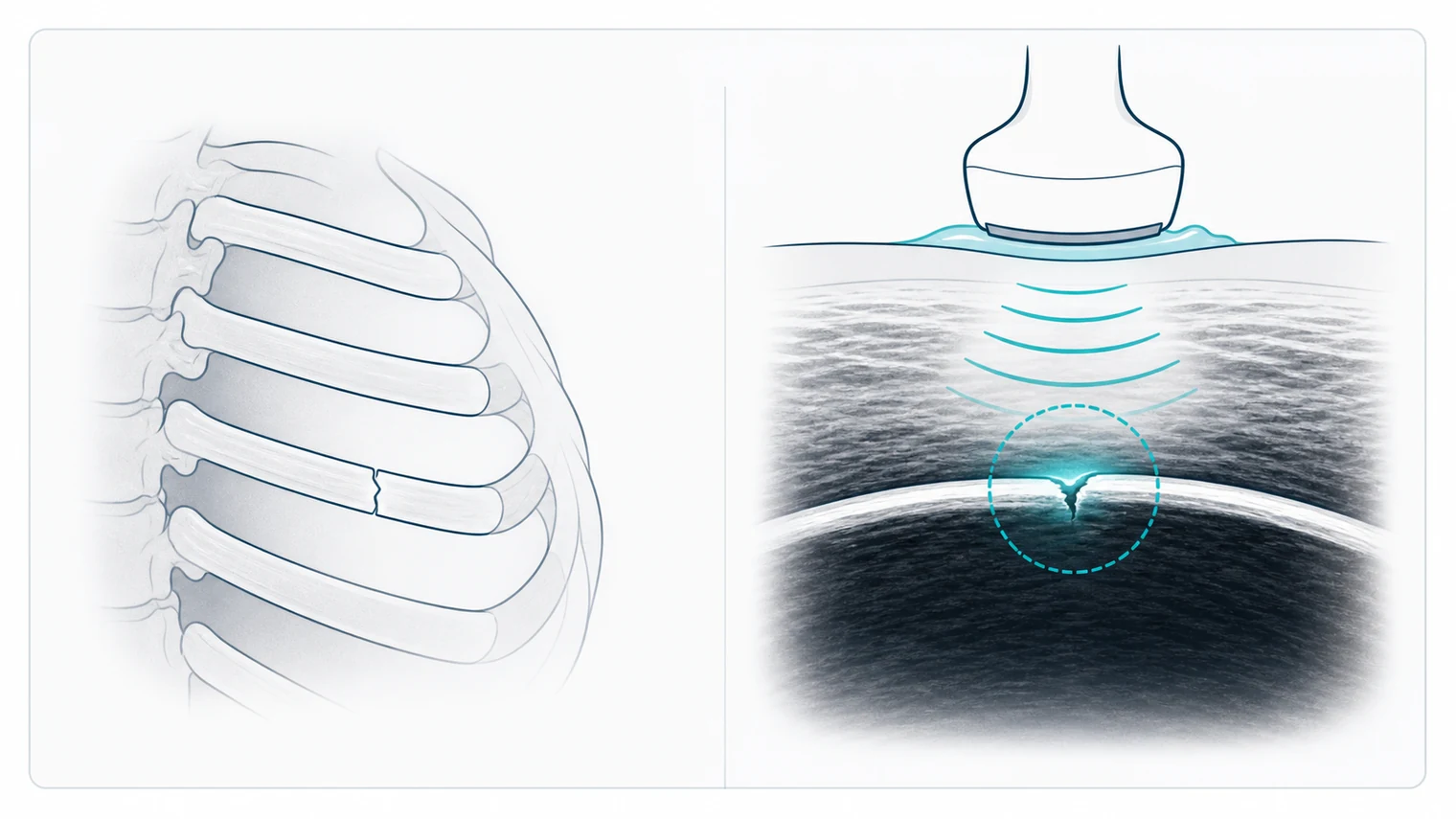
Ribs: The Ones X-Ray Misses
Ribs are the headline example. They are notoriously hard to read on X-ray, and a non-displaced rib fracture often does not show up at all.
The figure that surprises people. Ultrasound has been shown to detect nearly all rib fractures, compared with less than half picked up on a normal X-ray. A non-displaced rib fracture usually keeps its periosteum intact, which is exactly the setup that produces a clear periosteal lift and blood collection on ultrasound.
There is not much to actively do about a cracked rib. But knowing is its own kind of relief, and that came through in the cases Tabitha shared.
The Traps
None of this works without knowing your anatomy, because plenty of normal things can masquerade as a fracture. Tabitha ran through the usual traps:
| Looks like a fracture | What it actually is |
|---|---|
| Small irregularities on the bone surface | Normal vascular channels, which light up with colour Doppler |
| A separate bony fragment | An accessory bone or ossicle, usually with smooth, well-rounded edges |
| A gap in the bone in a child | A normal growth plate, which is why paediatric anatomy has to be known cold |
| A bony bump near a joint | An osteophyte from old wear and tear, not a new break |
A real fracture tends to have sharper, more irregular edges, and crucially it brings those secondary signs with it: the periosteal reaction, the swelling, the increased blood flow. When in doubt, compare with the other side or the next bone along.
One pattern she singled out for paediatric trauma is worth repeating:
"Really, with these paediatric patients that have had trauma, it's almost never a tendon issue, it's always a bone issue."
– Tabitha Gosden, sonographer, Ultrasound Insight
Real Cases
The case studies made the point better than any theory. A few of them:
- A seven-year-old with arm and elbow pain after a fall. The X-ray the next day was read as normal, and she was sent for a suspected tendon problem. The scan showed a clear blood collection in the elbow joint and the secondary signs of a fracture. Looking back at the X-ray afterwards, the break had been there all along, just overlooked.
- A six-year-old with shoulder pain after a fall, again with a normal X-ray and a tendon referral. The scan found a tiny break tucked on the underside of the collarbone, surrounded by swelling and increased blood flow.
- An eighteen-year-old with ongoing pain weeks after an injury, who had already had a normal abdominal scan and chest X-ray. Asked to point to the sore spot, she led straight to an anterior rib fracture that was starting to heal.
- A twenty-five-year-old with lateral foot and ankle pain after rolling his ankle, referred for a ligament injury. The scan showed an obvious break right through the fifth metatarsal.
The thread running through all of them is the same: do not lean too hard on the referral or the earlier report. Ask the patient where it hurts, and have a look.
"Just doing an abdo, it takes two minutes to ask them, where are you sore? Have a quick run over, and sometimes you find stuff."
– Tabitha Gosden, sonographer, Ultrasound Insight
Why It Matters
Ultrasound will not catch every fracture, and it is not here to replace X-ray or CT. What it does well is rule a fracture in quickly, with no radiation, while also showing the soft tissue and letting the sonographer watch the area move. For a child, or for anyone where radiation is a concern, that is a real advantage.
The other message from the session was about confidence. It is easy to defer to the X-ray report and move on. But the secondary signs are often right there on the screen if you look.
"Don't get caught up in the limited details on the referral. Be confident in what you're seeing. And when you do find these, you just feel really smart."
– Tabitha Gosden, sonographer, Ultrasound Insight
For patients, the practical takeaway is simple. If you are still sore in one specific spot after a fall, and the X-ray came back clear, it is reasonable to ask whether an ultrasound might add anything. Sometimes it finds the answer that explains the pain.
Want a mobile ultrasound that comes to you?
For Home Visits:
Book Home Ultrasound – assessment in your own space
For Aged Care Facilities:
Book Facility Visit – bedside imaging without a hospital transfer
Important note: This article summarises an educational talk and is for general information only. It is not a diagnosis or medical advice. The quotes are transcribed from a recorded session and lightly edited for clarity. If you have had an injury and are worried about a fracture, please see your GP or present to your nearest emergency department.