Your hands feel stiff and swollen first thing in the morning, and it takes a while before the fingers loosen up. Maybe it comes and goes. Maybe someone has waved it away as "a touch of arthritis" and left it there. Here is the part worth knowing before you shrug it off too: arthritis is not one condition, and some of the types behind that stiffness are very treatable when they are caught early.
At the Australasian Sonographers Association (ASA) 2026 conference on the Gold Coast, two presenters shared the stage for a session on ultrasound in rheumatology: Dr Maxine Szramka, a rheumatologist, who covered what is actually going on inside a sore joint and how it is treated, and Jennifer Garner, a sonographer and ultrasound educator, who explained where imaging fits in and how to scan for it. Between them they walked through something most people never get to see: how a swollen, sore joint is worked up, and where ultrasound comes into the picture. We have pulled the most useful parts together here, with their words quoted directly.
The short version, whether you have ongoing joint pain or you scan joints for a living: inflammatory arthritis is common, it is treatable, and ultrasound can catch it early, often before anything shows up on an X-ray. The sooner it is caught, the better people tend to do.
The quick version
- There are more than 100 types of arthritis, and the treatment depends entirely on which one you have.
- Rheumatoid arthritis is a whole-body inflammatory disease, not just sore joints, and it can affect people of any age.
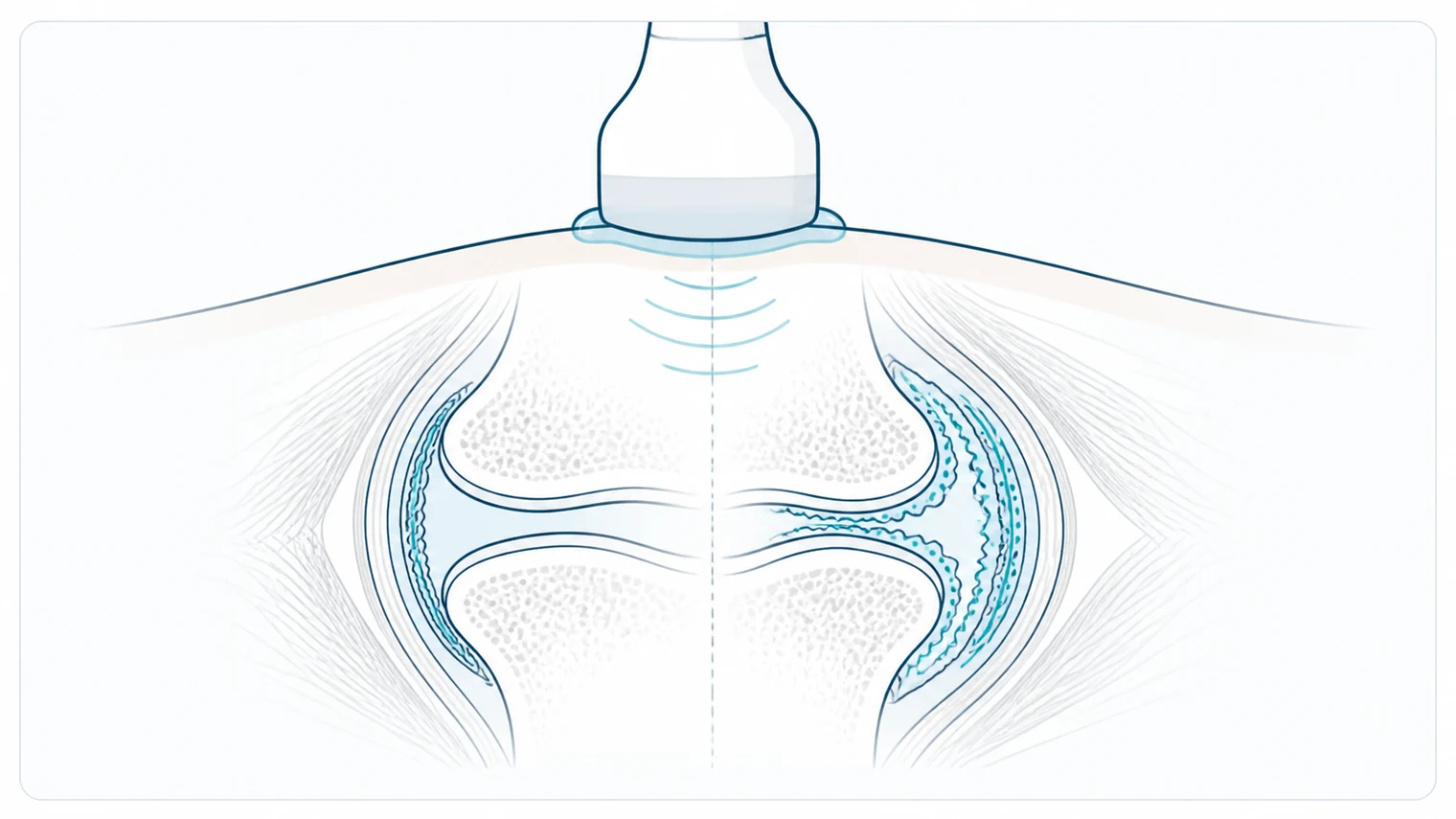
- Ultrasound looks for synovitis, tenosynovitis, effusions and early erosions to help tell inflammatory causes apart from mechanical ones.
- Getting onto treatment within about six weeks gives people far better long-term outcomes.
What a Rheumatologist Actually Does
Most people are a little hazy on what a rheumatologist treats. The rheumatologist who opened the session, Dr Maxine Szramka, put it plainly: they are arthritis experts who diagnose and treat every type of arthritis, along with autoimmune connective tissue diseases like lupus, the various forms of vasculitis, and a long tail of conditions that leave people unwell without an obvious cause.
"If someone's really sick, they're tired, they've got rashes, a lot of pain in their body, weird stuff going on and no one really knows what's happening, they'll come and see people like us. We do a full and comprehensive assessment, ask a lot of questions, try to make things simple, and then organise tests."
– Dr Maxine Szramka, rheumatologist
A lot of that detective work is about pain. Where is it, why is it there, and what is driving it, because pain in one part of the body can have a completely different cause to pain somewhere else. That distinction matters, because the treatment for inflammatory pain is nothing like the treatment for mechanical pain. Imaging, including ultrasound, is one of the tools used to tell them apart.
More Than 100 Types of Arthritis
Here is the part that surprises people. "Arthritis" is not one disease.
"A lot of people think arthritis is synonymous with osteoarthritis, or with rheumatoid arthritis. But there are actually more than 100 different causes of arthritis, and it's really important to get the diagnosis correct, because the management needs to be tailored to the cause."
– Dr Maxine Szramka, rheumatologist
The common ones came up again and again during the talk. Here is how they were described.
| Type | What sets it apart |
|---|---|
| Rheumatoid arthritis | The one everyone pictures. Inflammation and fluid in the joints, usually (not always) symmetrical. |
| Psoriatic arthritis | Inflammatory like rheumatoid, but linked to the skin condition psoriasis, and it behaves and responds a little differently. |
| Osteoarthritis | The degenerative, wear-and-tear type. You can have it without pain, and pain without it. Increasingly understood as primarily a bone problem. |
| Ankylosing spondylitis | Inflammatory arthritis affecting the spine and the entheses (where tendons meet bone), sometimes the peripheral joints too. |
| Gout and pseudogout | Crystal arthritis. Different crystals, similar misery, and very treatable. |
The point of naming them is not trivia. Each one is managed differently, so the diagnosis decides the treatment. That is exactly why a clear picture of the joint is worth so much.
Rheumatoid Arthritis in Plain English
Rheumatoid arthritis is a systemic inflammatory condition. It does not just affect joints. It can bring on fevers, fatigue and weight loss, and over time it can touch the lungs, the heart, the skin, the eyes and the bones.
A few things tend to catch people out. It is usually symmetrical, affecting the same joints on both sides, but not always. It is not just an older person's disease either. Around half a million Australians were estimated to have it in 2022, it affects women about twice as often as men, and it can appear in children as well as adults.
It also varies enormously in how it shows up, which is part of why it gets missed.
"Some people can have inflammation without pain. Others present with high fevers, swollen joints and so much pain you think they've got an infection. And some people have really low-grade symptoms for years without even noticing, then you investigate and find they've had low-grade arthritis for five to ten years and never knew."
– Dr Maxine Szramka, rheumatologist
The encouraging part is how much has changed. The crippling, deforming rheumatoid arthritis that once filled hospital wards is now rare, because treatment has been transformed over the past few decades. Most people lead normal lives. Around half go into remission on methotrexate alone, and many of the rest do well on a combination of older oral medications, with biologics and other targeted drugs held in reserve for those who need them.
Where Ultrasound Comes In
This was the question Jennifer Garner set out to answer: rheumatology over here, ultrasound over there, so where do they meet? The honest answer is that they meet in the joints, tendons and entheses, and the scan is there to help with one decision above all.
"Is it an inflammatory condition or a mechanical one, and therefore how are we going to treat it? The conditions that are mechanical, that don't need our drugs, can present similarly, and ultrasound and MRI can be really key in helping us decide."
– Jennifer Garner, sonographer
So what is the scan actually looking for? A handful of findings come up over and over:
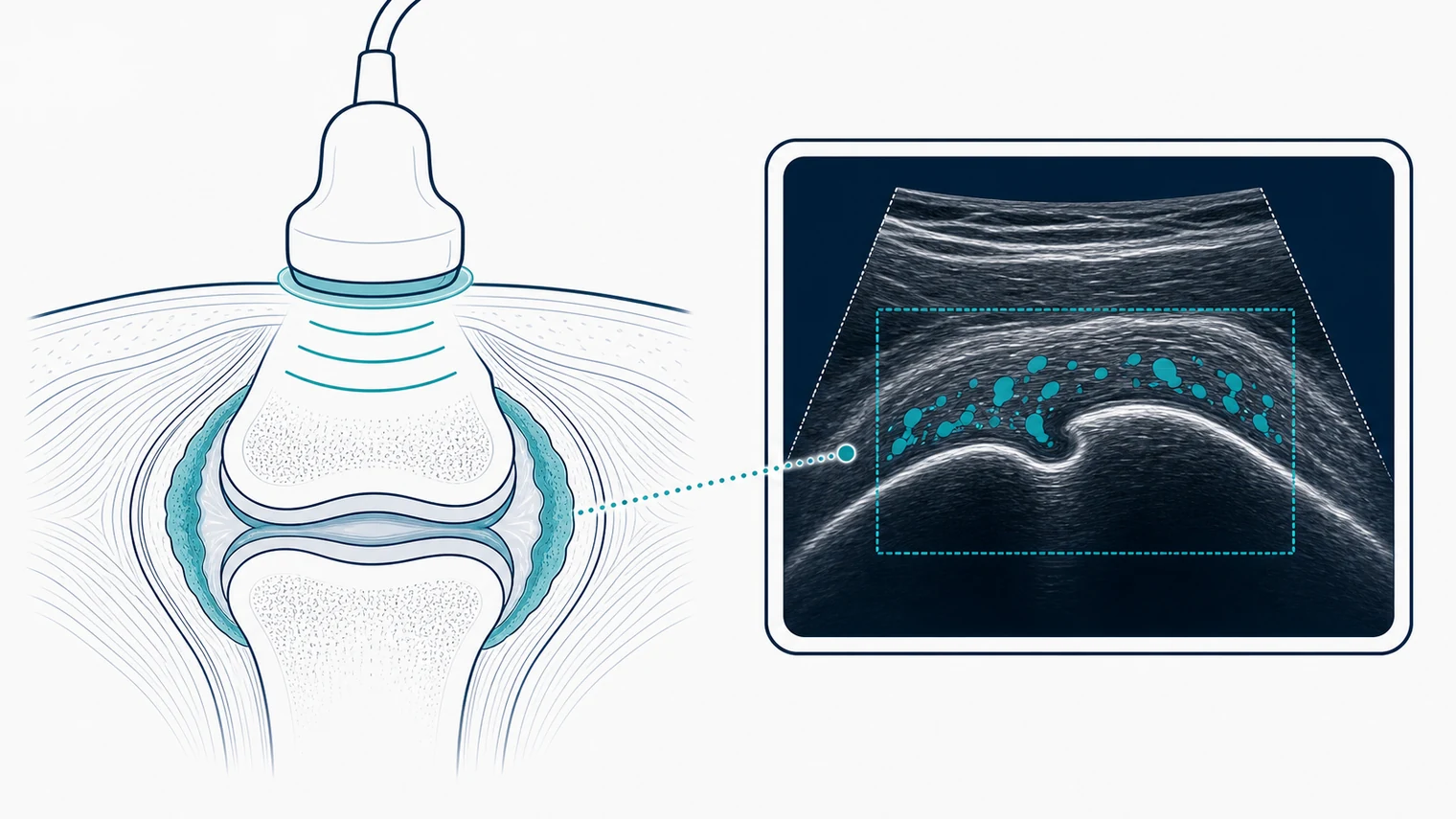
- Synovitis – a thickened, inflamed joint lining, often with increased blood flow on Doppler. This is the core sign of joint inflammation.
- Tenosynovitis – inflammation around a tendon. This one is important, because inflammatory arthritis can hit the tendons first, before the joints ever swell.
- Effusion – fluid in the joint, and the type of fluid can hint at gout versus a simple effusion.
- Bursitis – which can be purely mechanical, but in the right clinical picture can be an early flag for inflammatory disease.
- Bone erosions – small punched-out defects at the joint margin, a sign of damage that ultrasound can sometimes pick up earlier than plain X-ray.
That tendon point is worth sitting with, because it is the kind of subtle finding that changes a diagnosis.
"If you have multifocal tenosynovitis, that's an alarm bell. People do not always present with swelling in the joints. Subtle findings, in the context of the clinical situation, help us treat people better."
– Dr Maxine Szramka, rheumatologist
How gout looks different. On ultrasound, gout tends to show bright deposits sitting on the surface of the cartilage, the so-called double contour sign. Jennifer reached for a food analogy to keep it memorable: ordinary gout is like a thick layer of Vegemite on the surface of a sandwich, while pseudogout, with calcium sitting inside the cartilage itself, is more like a lamington. Odd, but it sticks.
There is also a reason that goes beyond the diagnosis itself. A clear scan gives the patient a solid foundation, evidence they can see, which matters when the treatments carry real risks and need genuine informed consent.
Which Joints, and How Much
If you scan, you will know the next problem well. The published frameworks, EULAR (the European Alliance of Associations for Rheumatology) and OMERACT (Outcome Measures in Rheumatology), describe scoring systems and joint counts that can run to 48 or even 78 joints. It is easy to freeze and wonder where to even start.
Jennifer's advice was refreshingly direct: keep it simple.
"Go for synovial thickening in the joint, tenosynovitis, enthesitis, and any bone erosions. How many, how big, and which ones are affected. Put some colour on with a low-flow setting. And have a conversation with your rheumatologist or radiologist about what they actually want."
– Jennifer Garner, sonographer
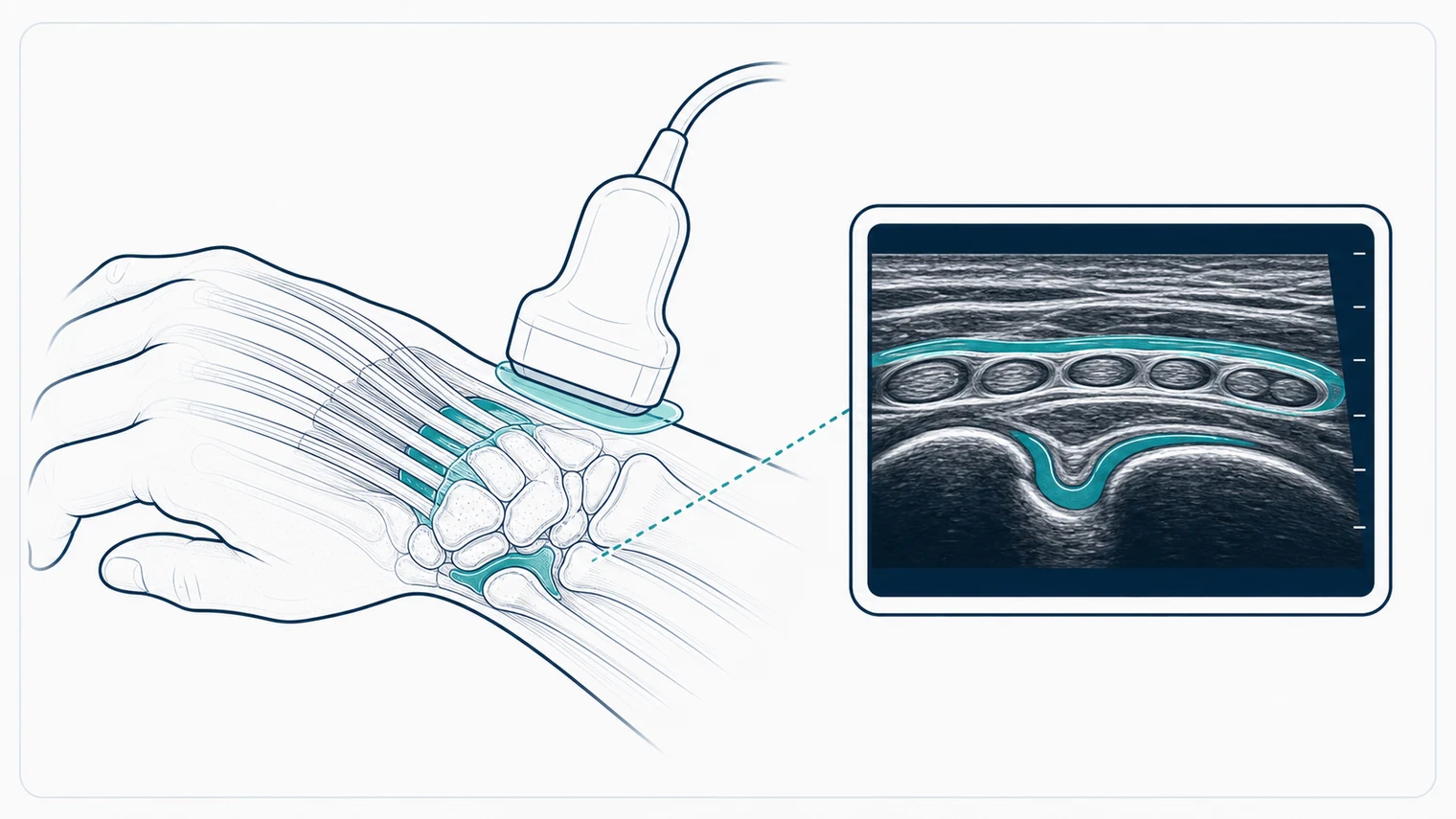
The practical routine she demonstrated on a wrist ran along familiar lines: check the radiocarpal joint for effusion and synovial thickening, sweep the extensor tendons in cross-section for tenosynovitis, add power Doppler or a sensitive low-flow mode with a light touch on the probe, then work down to the metacarpophalangeal joints, bending each finger to expose the bone and look for erosions in two planes. Compare sides when one looks inflamed. The detail can be scored later if needed; the priority is spotting whether inflammation is there at all.
Why Six Weeks Matters
The single most important message from the rheumatology side was about time.
The window that changes outcomes. Studies have shown that starting treatment within around six weeks of inflammatory arthritis appearing leads to far better long-term results. That is why a prompt, accurate scan is not just a tick-box. It can move someone onto effective treatment weeks earlier, and those weeks count.
Maxine's clinic builds its whole schedule around that idea, working longer hours and Saturdays to see new inflammatory arthritis referrals within a few weeks. Imaging is part of what makes early, confident decisions possible.
So if you have joints that are stiff or sore, especially first thing in the morning, the takeaway is simple. Do not sit on it.
"If there's any stiffness, any pains, I'm super encouraging people to at least come in and get an assessment. That can change the outcome of your life."
– Dr Maxine Szramka, rheumatologist
Ultrasound is one of the quietest, lowest-stress ways to start answering the question. No radiation, no contrast, and you can watch the joint move in real time. For someone who finds it hard to get to a clinic, having that scan come to them removes one more reason to put it off.
Want a mobile ultrasound that comes to you?
For Home Visits:
Book Home Ultrasound – assessment in your own space
For Aged Care Facilities:
Book Facility Visit – bedside imaging without a hospital transfer
Important note: This article summarises an educational talk and is for general information only. It is not a diagnosis or medical advice. The quotes are transcribed from a recorded session and lightly edited for clarity. If you have joint pain or symptoms that worry you, please see your GP or specialist.